
In an era where weight loss medications such as Semaglutide are increasingly in short supply, the intragastric balloon continues to be a popular option for Class 1 obesity patients (who wish to lose only 10 or 20kg). Bariatric and laparoscopic Surgeon Mr Jason Winnett answers GPs most asked questions.
Intragastric balloon versus weight loss injections – which patients are suitable?
The Orbera® Intra Gastric Balloon (IGB) is increasingly popular with Class 1 obesity patients who wish to lose 10-20kg. I frequently perform this procedure for those wanting to lose post-pregnancy baby weight.

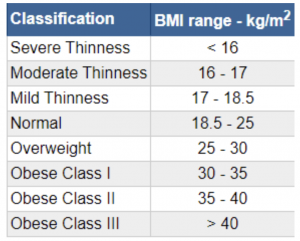
Suitable patients include those with a BMI of 27-35 kg/M2, plus or minus comorbidities (e.g. arthritis, venous stasis disease, high cholesterol, hypertension, diabetes, fatty liver syndrome and gallbladder disease).
Patients not suitable for the IGB include:
- Patients under 18
- Patients who have had previous upper gastrointestinal surgery
- Patients who regularly take aspirin, non-steroidal anti-inflammatory agents, COX-2 inhibitors, anti-coagulants or anti-platelet agents
- Pregnant patients
- Patients with clinically significant hiatus hernia
- Patients with a history of inflammatory disease of the gastrointestinal tract
- Increasingly, for morbidly obese patients with very high BMIs, the balloon can also be used as a preliminary procedure to help patients lose weight before surgery in order to reduce liver volume and better facilitate a bypass or sleeve surgery.
Semaglutide is a subcutaneous weekly weight loss injection with a starting dose of 0.25mg, increasing after 2 weeks to 0.50mg, then 4-weekly increases as tolerated to 0.75mg/1.0mg weekly. Currently, it is only approved for Type 2 diabetes but used off-label for obesity. Contraindications include medullary thyroid cancer and multiple endocrine neoplasia 2.
Semaglutide also achieves good short-term weight loss, but weight almost always returns when medication stops.
The balloon is generally very safe; however, extremely rare complications, such as a leak, may occur. Medication remains a safer option as it can simply be discontinued with any side effects.
Semaglutide is generally well tolerated, and has also recently been cleared of any links to suicidal thoughts in a large study of 10,000 plus patients.
GPs may consider referring to a weight specialist who can assess the most suitable option and provide advice on the best treatment, along with information on potential risks or complications.
What is the metabolic efficacy of the Intragastric balloon procedure in the short-term?
Several metabolic parameters and medical comorbidities are improved in the short-term in patients who utilise IGBs, compared to diet and exercise alone.
Pooled data from five clinical trials and 18 observational studies illustrates that IGB lowers both HbA1C and fasting blood glucose (FBG) more than non-invasive options, with particular benefits in patients with FBG greater than 100 mg/dl or HbA1C more than 6.5%. Mixed results were shown with respect to improving patient’s lipid profiles.
While no benefit was observed in reducing triglycerides for those patients who used IGB therapy, there was a decreasing trend of low-density lipoproteins in obese patients using IGBs.
Improving liver function test abnormalities are also observed in patients who use IGBs for weight loss with ALT values decreasing by 9 U/I and AST values lowering by 3 U/I.
Finally, diabetes, hypertension and dyslipidaemia all achieved remission to a statistically significant greater degree in patients who utilised an IGB for weight loss as opposed to those patients who pursued a non-invasive approach.
Taken together, current data suggests that IGB therapy improves laboratory abnormalities and medical diseases associated with obesity to a better degree than lifestyle modifications alone.
What about the long-term results for Intragastric balloon?
At least one small study in the Journal of Obesity and Eating Disorders shows that about 25% of people maintained weight long-term, and the remaining patients experienced partial or full return of weight within 1 to 4 years after removal.
It also found that success of IGB likely requires early intensive lifestyle adjuncts can be a valuable bridge in the short-term as a bridge to sustainable medical or surgical weight-loss programs.
What is involved in the IGB procedure?
There is no general anaesthetic involved and the patient is given a mild sedative using endoscopic equipment to place the balloon, which is then filled with saline in a 20-minute procedure. The balloon is generally removed in 6-12 months’ time, in the same way.
What is the IGB recovery like?
Most people have little to no appetite after the balloon is inserted and are restricted to a liquid diet for 14 days, followed by a puree diet. Commonly, patients will lose 2-6kg in the first week. About 90% of the weight loss will occur in the first 3 months, with the next three months primarily focused on maintenance.
The balloon is generally removed after 6-12 months as a day procedure. Most patients are back to work and exercising in 4 to 5 days.
What are important considerations for GPs after the IGB?
- It is important that patients take a complete multivitamin and mineral supplement with Iron, and a separate Calcium and Vitamin D supplement, as it is more difficult to meet the requirements following insertion of the balloon.
- Patients should be reviewed at two weeks post-insertion, then three monthly.
- Common side effects are crampy stomach pain and vomiting for the first few days, which requires slow progression with drinking and eating, and anti-nausea medication.
- Red flags include persistent nausea, acid reflux, leakage (rarely occurs, but the balloon contains a dye, which will show up as blue/green in urine/vomit or stools to indicate removal is necessary).
- Serious side effects are rare and include migration (1.4% of cases), small bowel obstruction (0.3%), and perforation (0.1%). Intestinal obstruction may occur rarely due to balloon deflation with subsequent distal migration, although most are expelled from the rectum.
- Risk of stomach ulcer is rare, and PPI therapy is to be continued until removal.
- The device is not permanent and is effectively a teaching aid to help patients develop healthy eating habits.
- The average weight loss is 10-15kg with the six-month balloon and 15-25kg with the twelve-month balloon; however, it is highly variable for each individual patient.
IGB in the short term is about 3 times the weight generally lost with diet and exercise alone. At Winnett Specialist services, all of our patients receive a customised diet and exercise program and support in making healthy lifestyle choices to encourage portion control. If you have questions or would like to receive professional advice, please feel welcome to book a consultation with us.

Mr Jason Winnett
Laparoscopic and Bariatric Surgeon
P (03) 9417 1555
admin@winnettspecialistgroup.com.au
www.winnettspecialistgroup.com.au
Queens Terrace, 382 Victoria Parade, East Melbourne 3002
References:
Mayo Clinic Intragastric Balloon


{kind=link}
{kind=link}
{kind=link}