
You’ve done your research on weight-loss surgery. Now comes the big question: which surgery is right for you?
‘Most patients come to me with the same two worries: which procedure will give them optimal weight-loss results, and which one is suitable for them,’ says Melbourne-based bariatric surgeon Dr Jason Winnett.
In this guide, Dr Winnett will break down the benefits and risks of the three most common weight-loss procedures: gastric sleeve surgery, gastric bypass (Roux-en-Y) and mini gastric bypass.
Weight-loss surgeries at a glance
| Category | Gastric Sleeve | Gastric Bypass (RYGB) | Mini Bypass (OAGB) |
| How it works | Reduces stomach size by 80% | Reduces stomach to smaller pouch and bypasses part of short intestine | Creates narrow stomach tube and bypasses approx. 2m of bowel |
| Reversible? | No | Mostly no | Partly |
| Weight-loss potential | Strong | Very strong | Very strong |
| Biggest risk | Heartburn (reflux) | Low nutrients, dumping | Bile reflux, low nutrients |
Gastric sleeve surgery (sleeve gastrectomy)
In Australia, 79.8% of all primary weight-loss procedures performed in 2023 were sleeve gastrectomies, according to the Bariatric Surgery Registry.
In the same national data, primary sleeve gastrectomy had an adverse event rate of under 2%.
How does gastric sleeve surgery work?

Dr Winnett says: ‘During the procedure, surgeons remove around 80% of the stomach and shape the remaining portion into a slim, banana-shaped and banana-sized “sleeve”, much smaller than the pouch you started with.
‘Sleeve gastrectomy is performed laparoscopically (keyhole surgery) through five or six small cuts in the abdomen, with a shorter operating time and a lower technical complexity than many other bariatric procedures.
‘The sleeve does not involve rerouting the intestines, so the normal pathway of food through the bowel is preserved. That means typical nutrient absorption remains largely intact, which may reduce the risk of some severe malabsorption‑related deficiencies compared with more complex bypass procedures.’
Risks and side effects of gastric sleeve surgery
Dr Winnett says that after sleeve gastrectomy, 10% of patients develop new or worsening Gastroesophageal reflux disease (GERD), but this is markedly reduced by repairing a hiatus hernia at the time of surgery.
‘GERD occurs when stomach acid repeatedly flows back up into the oesophagus, causing burning pain in the chest (heartburn), and sometimes coughing or difficulty swallowing,’ says Dr Winnett.
‘That’s why careful screening is important. Although usually treatable through lifestyle measures and proton pump inhibitors, a small number of patients eventually need further treatment or conversion to another procedure because of severe, persistent GERD.’
Strictures – a narrowing of the new, narrow stomach tube that makes it hard for food and even liquids to pass through – are uncommon but recognised complications of gastric sleeve surgery.
Sleeve gastrectomy patients also need to take daily nutritional supplements for life, including iron, B12, Vitamin D, folate, zinc, thiamine, and magnesium.
Read more about gastric sleeve surgery.
Mini gastric bypass surgery
Also known as one anastomosis gastric bypass (OAGB).
In the 2023 Australia and New Zealand Bariatric Surgery Registry, mini gastric bypass accounted for about 10.9% of all primary bariatric procedures behind sleeve gastrectomy (79.8%).
How does mini gastric bypass surgery work?
Mini gastric bypass is a modern type of weight‑loss surgery that combines a smaller stomach with a simple bypass of the small intestine.
‘The surgeon creates a long, narrow stomach pouch,’ says Dr Winnett, ‘and connects it to a loop of small bowel further down. Food passes from the small pouch straight into the intestine and skips the rest of the stomach and the first part of the bowel.
This helps weight loss in two main ways:
- The stomach feels full after much smaller meals
- The body absorbs fewer calories after eating
Risks and side effects
One possible side effect is reflux. ‘Because food and bile share the same loop of bowel going into the small stomach pouch, bile can more easily wash back into the pouch and sometimes up towards the oesophagus,’’ says Dr Winnett.
A study in the Annals of Medical Surgery 2021 reports that signs of bile reflux after OAGB are seen in a noticeable minority of patients.
‘In a small number of patients, this can cause persistent burning and bitter fluid coming up, which may require medication or even conversion to a Roux‑en‑Y gastric bypass,’ says Dr Winnett.
Mini gastric bypass patients need to be on daily nutritional supplements for life including iron, B12, Vitamin D, folate, zinc, thiamine and magnesium.
Read more about mini gastric bypass surgery (OAGB).
Gastric bypass surgery (Roux-en-Y)
The classic Roux-en-Y bypass (RYGB) is a procedure that has been performed for decades and remains one of the most well-studied weight-loss surgeries in the world.
In Australia, about 8.6% of all primary bariatric procedures recorded in 2023 were Roux‑en‑Y gastric bypass operations.
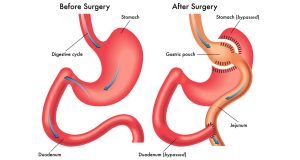
How does gastric bypass surgery (Roux-en-Y) work?
During the procedure, the stomach is divided to create a small upper pouch, roughly the size of an egg, and connected directly to the lower section of the small intestine. The rest of the stomach, along with the first part of the small intestine, is bypassed completely.
Like the mini gastric bypass, it helps the stomach feel full more quickly, and it means the body absorbs fewer calories.
‘It’s a more complex procedure than the mini gastric bypass, with two connections instead of one in the bypass,’ says Dr Winnett.
Risks and side effects
Stomal stenosis (narrowing at the join): The small pouch can become too tight, causing nausea, vomiting or food ‘sticking’. This is often treated by stretching the area with an endoscope.
Dumping syndrome: Some people experience flushing, dizziness, shakiness or diarrhoea when sugary or rich foods empty too quickly into the small bowel. This usually improves with slower eating and lower‑sugar, higher‑protein foods.
‘Like gastric sleeve patients, bypass patients also need to be on daily nutritional supplements for life,’ says Dr Winnett.
Read more about gastric bypass surgery (Roux-en-Y).
Weight-loss potential – how does each procedure compare?
In a 2024 Lancet study of 628 patients, those who had a Roux‑en‑Y gastric bypass achieved significantly greater total weight loss than those who had a sleeve gastrectomy, and also showed better improvement in obesity‑related problems, such as abnormal blood lipids and gastro‑oesophageal reflux disease (GERD).
And what about the results between the two bypass procedures?
According to a 2025 Obesity Surgery Journal study, patients achieved longer-lasting results with mini gastric bypass (OAGB) than with Roux-en-Y.
It found OAGB may offer greater total weight loss within a shorter operative time, while RYGB may be more suitable for patients with severe reflux.
‘Ultimately,’ says Dr Winnett, ‘the surgical profile of each patient is different and requires careful assessment with your GP and surgeon.
Which weight-loss procedure is best for you?
According to Dr Winnett:
- Gastric sleeve surgery is often the preferred surgery for uncomplicated weight loss.
- Gastric bypass (Roux-en-Y) is often chosen for people with severe obesity, severe reflux or Type 2 diabetes, and may notably improve these conditions.
- Mini gastric bypass (OAGB) is a shorter, simpler surgery with similar weight-loss results but suited to patients with a lower reflux risk.
The right procedure depends on your individual health, weight history and goals. A thorough medical assessment is the only way to know which option suits you.
At Winnett Specialist Group, Dr Winnett and his team will assess your situation and talk you through the procedure best suited to your needs.
Book a consultation with our team.
References
- Fewer Australians having bariatric surgery: Monash University-led report Does Sleeve Gastrectomy Expose the Distal Esophagus to Severe Reflux?: A Systematic Review and Meta-analysis – PubMed
- 2 Two-year outcomes of sleeve gastrectomy versus gastric bypass: first report based on Tehran obesity treatment study (TOTS) – PMC
- Does Sleeve Gastrectomy Expose the Distal Esophagus to Severe Reflux?: A Systematic Review and Meta-analysis, Annals of Surgery 2020.
- Bile reflux after one anastomosis gastric bypass surgery: A review study, Annals of Medical Surgery London, 2021
- Long-term effect of sleeve gastrectomy vs Roux-en-Y gastric bypass in people living with severe obesity: a phase III multicentre randomised controlled trial (SleeveBypass) – The Lancet Regional Health
- Comparative Effect of Roux-en-Y Gastric Bypass vs. One-Anastomosis Gastric Bypass for Revisional Surgery After Sleeve Gastrectomy With Insufficient Clinical Response: A Systematic Review and Meta-analysis – Obesity Surgery Journal 2025.
Reviewed April 2026 by Dr Jason Winnett
AHPRA Registration MED0001155541
* Bariatric surgery carries risks, individual results vary and every patient’s journey is different. This article is for general education only, not personal medical advice. Always follow the guidance of your surgical team.
Contact
P (03) 9417 1555
admin@winnettspecialistgroup.com.au
www.winnettspecialistgroup.com.au
Queens Terrace, 382 Victoria Parade, East Melbourne 3002



{kind=link}
{kind=link}
{kind=link}