
1. The Mini Gastric Bypass is here for good
Gastric Sleeve surgery (or Sleeve Gastrectomy) is the “go to surgery” for uncomplicated obesity or type 2 diabetes.
Traditionally, for patients with obesity who also have diabetes, the Roux-en-Y-Gastric Bypass has been for years the ‘gold standard’ for longer-term diabetes remission. But the Mini-Gastric Bypass has now proven to be highly effective as well.
“The 2022 Bariatric Surgery register shows that 70% of all insulin-dependent patients were off insulin within a year of surgery, irrespective of the type of whether it was sleeve, bypass or the Mini Gastric Bypass,” says Melbourne Bariatric and Laparoscopic Surgeon Mr Jason Winnett.
“However, the Mini Gastric Bypass is now also clinically proven to have better long-term diabetes remission without medication than the Sleeve,”
Mr Winnett says the Mini-Gastric Bypass is a simpler procedure, taking about 50 minutes less time on the table. As a result, the anaesthetic risks and complications are lower than those associated with standard bypass surgery.
“Also, revision surgery can be performed if it needs to be reversed on a Mini–Gastric Bypass.
“However, with the standard bypass, revision surgery is very complicated and normally only done when no other options exist.”
He also says that patients who have a Mini-Gastric Bypass tolerate a wider variety of foods more than the standard bypass.“However there is no one-size-fits all. On the upside for the regular Bypass is more suitable for patients with severe gastro-oesophageal reflux or oesophageal dysmotility.”
GP investigations before any bariatric surgery include
- Routine labs: fasting lipids, full blood count, urea and electrolytes, liver function tests, coagulation screen, urinalysis, fasting glucose and glycated haemoglobin (HbA1c) to screen for diabetes).
- C-peptide level to predict diabetes remission.
- Nutritional screen: iron studies, vitamin B12 folate 25-OH, vitamin D.
- Gastrointestinal evaluations such as abdominal ultrasound and endoscopy may be required.
- Electrocardiogram and polysomnography may be required if cardiovascular or sleep apnoea is suspected.
- Psychiatric evaluation and psychiatry referral if known or suspected psychiatric illness or substance abuse.
While there are no absolute contraindications to bariatric surgery today, relative contraindications exist for more extensive surgeries like sleeve and bypass. These include conditions such as heart failure, unstable coronary artery disease, end-stage lung disease, drug and alcohol dependency, impaired intellectual capacity, and Crohn’s Disease (for BYPASS).
Source: 2022 Bariatric Surgery Registry Annual Report Summary.
2. Safety profile for bariatric surgery is similar to many standard operations
Bariatric surgery today has an excellent morbidity and mortality profile, with similar risk profile to knee replacement or appendectomy,” according to a December 2023 report in the Surgery for Obesity and Related Diseases.
And since Australia’s own Bariatric Surgery Registry started more than a decade ago, surgeons across Australia have performed 157,909 surgeries with 54 deaths recorded within 90 days of surgery (0.03% risk).
“The mortality and morbidity risk is important of course. But this is almost negligible compared to the lives of almost certain disability and often premature death if patients don’t have the surgery.”
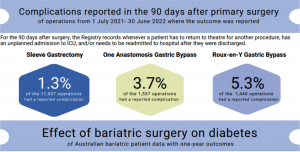
He says in terms of popularity, 8 out of 10 patients had sleeve surgery in 2022 (11, 907 procedures), compared with 1,537 mini-gastric bypass procedures and 1440 Roux-en-Y Gastric Bypass procedures.
Complication rates for Sleeve Gastrectomy were 1.3%, 3.7% for the Mini Gastric Bypass and 5.3% for the Gastric Bypass.
For GPs, he says the main complications of Sleeve Gastrectomy include staple line leak, gastroesophageal reflux, dilatation of the gastric remnant and weight regain.
For both bypass surgeries, issues tend to be nutritional absorption issues, longer recovery time and more chance of dumping than the Sleeve.
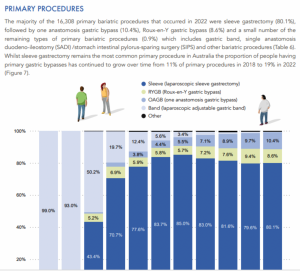
The registry report shows that there were 16,308 primary procedures performed in 2022 and that:
- 80.1% were Sleeve Gastrectomy
- 86% of patients were female
- 43.5 years was the average age at operation for primary procedures
- 27.4% was the average total weight loss at one-year following a primary bariatric procedure
- 10.4% were one anastomosis Mini-Gastric Gastric Bypass
- 8.6% were two anastomosis Roux-en-Y- Gastric Bypass
- 0.9% were “other” (including Laparoscopic Adjustable Gastric Band)
- 16.8% of patients were on insulin for diabetes at time of surgery
Source: 2022 Bariatric Surgery Registry Annual Report
3. Semaglutide cuts cardiac risk for patients, irrespective of diabetes status
New research on 17,000 patients reported in the GP publication AusDoc shows that adding Semaglutide to standard care cuts the risk of fatal and non-fatal cardiac events by 20% in adults with pre-existing cardiovascular disease but not diabetes.
But unfortunately the shortage continues…
“The Semaglutide shortage is expected to continue into 2024,” says Mr Winnett.
“And on top of that shortage, now dulaglutide is in short supply as well.”
Mr Winnett adds that for other chronic conditions like severe obesity, the TGA has now approved the temporary supply of overseas-registered Semaglutide products which pharmacists can order from the following companies:
- Medsurge Healthcare call 1300 788 261
- Pro Pharmaceuticals Group call 1300 077 674
Mr Winnett says other possible prescribing options for GPs during the shortage include:
- Liraglutide shown to have 6.4% effectiveness v 15% Semaglutide in one JAMA study. Contraindications include medullary thyroid cancer and multiple endocrine neoplasia 2 (the same for Wegovy and Ozempic).
- Phenteramine – Use sparingly. Is tolerable short-term but causes frequent dry mouth, palpitations, hypertension and insomnia. Some patients report that by varying the dose and missing a couple of days they have experienced better results, due to drug tolerance issues. Many patients use 15mg on alternate days, or 30mg weekdays only.
- Topiramate – Use sparingly. Is traditionally used for migraines and tension headaches, but also suppresses appetite. It can be used 25-50mg daily, or twice daily. Side effects include mood swings, blurred vision and suicidal thoughts.
- Combination naltrexone and bupropion – Use sparingly. This targets brain appetite but is linked to hypertension and seizures, constipation and suicidal thoughts.
Metabolic Medicine Explosion
Mr Winnett says that GPs can also expect to see “more and more” weight loss drugs come on the market in 2024.
Novo Nordisk, the company that makes Semaglutide and Wegovy, now has a market capitalisation that exceeds the Gross Domestic Product of its host country Denmark, according to a December media report in the SMH.
“We shall probably hear a fair bit more about Tirzepatide in 2024 too, with the NEJM recently concluding it can cause substantial and sustained body weight reduction after 72 weeks with weekly injections.”
As 2024 unfolds, GPs play an indispensable role in the dynamic realm of obesity management. The effectiveness of the Mini Gastric Bypass, along with insights into pre-surgical evaluations and the evolving safety profile of bariatric procedures, illuminates a path towards improved health. For additional insights, explore further at Winnett Specialist Group by clicking here.

Mr Jason Winnett
Laparoscopic and Bariatric Surgeon
P (03) 9417 1555 admin@winnettspecialistgroup.com.au
www.winnettspecialistgroup.com.au
Queens Terrace, 382 Victoria Parade, East Melbourne 3002
Sources:
Bariatric Surgery Registry Annual Report 2022
Bariatric Surgery Registry of Australia 2022 Summary
RACGP News GP Semaglutide Shortage Sparks Patient Demand
Beyond Ozempic How weight loss drugs could change the World, SMH December 2023.



{kind=link}
{kind=link}
{kind=link}